What is Fear-Avoidance?
Athletes who experience an injury often struggle with fear-avoidance once they are physically cleared to return to sports. Out of fear of pain or injury, fear-avoidance is when a person develops and maintains chronic pain due to avoiding certain motions or behaviors. “Fear-avoidance is a model that describes how movement and pain-related fear can impact the development and maintenance of chronic pain and increased sensitivity to pain,” pediatric psychologist Emily Stapleton, Psy.D., says. To avoid perceived pain or injury, athletes may believe they cannot complete some rehabilitation exercises and as a result, the athlete may:
- hesitate when completing exercises
- not put in effort
- hold back in training or competition
- increase their dependency on family, coaches or medical team
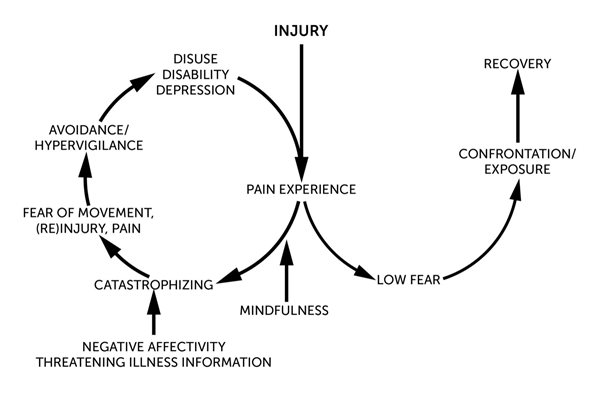
The more the athlete does these things, the greater the anxiety becomes about pain, movement and reinjury. This fear-avoidance cycle is shown below:
What Does Fear-Avoidance Look Like in the Athlete?
“In athletes, fear-avoidance may look like hesitation when completing necessary exercises for recovery or decreased effort in rehabilitation exercises,” Stapleton says. “You may also see athletes skipping certain physical therapy exercises, discontinuing exercises early, or not completing the number of reps or recommended time due to pain or pain-related fear. Outside of rehabilitation, athletes may avoid social activities or sports where they anticipate the need to engage in increased physical activity, or actions they perceive as unsafe or as likely to increase pain, such as walking long distances or standing for extended periods of time.”
Part of the fear-avoidance cycle includes catastrophizing, or assuming that the worst possible outcome or event will happen. “This pattern of thinking increases distress and is linked to both anxiety and depression,” Stapleton says. In athletes, catastrophizing can manifest in many ways:
- Constant or invasive thoughts about the pain of injury.
- The athlete might think their injury is the worst possible injury and that they will never get back to their pre-injury performance level.
- Believe nothing can be done about their pain or injury, and they will never recover.
This negative thinking can lead to fear of pain, movement, further injury and result in avoidance of anything that might cause pain, make the injury worse or result in another injury. As a result of increased anxiety and avoidance, one can become fixated on monitoring physical sensations in their body and very sensitive toward anything that increases discomfort, even physical therapy exercises that are needed for recovery. This often leads to sedentary behavior and will stop or greatly reduce physical activity levels. “Avoidant behavior is expected and healthy in the immediate acute phase post-injury, as following injury rest is often needed for recovery,” Stapleton says. “However, when returning to activities is appropriate or engagement in physical therapy exercises is necessary to recovery and rehabilitation, avoidance of these activities can actually be harmful, leading to increased pain, chronic pain, and/or declines in mood.”
In athletes, deconditioning often triggers more negative thoughts about their abilities, which can lead to depression and disability. Concerning signs and symptoms of depression include:
- changes in appetite
- changes in sleep
- irritability
- anger
- sadness
- frequent crying or emotional outbursts
- lack of motivation, a decline in academic performance
- disengagement and/or social withdrawal
- substance abuse
It is important to learn strategies to cope with the anxiety so that rehabilitation and recovery are not significantly impacted.
How to Provide Support
There are ways that you can help support your child and work through their range of emotions and fears:
- Help them to identify exercises or activities that increase negative emotions, or triggers. Look for when an athlete becomes distressed, avoids or hesitates prior to certain exercises for clues of triggering activities/exercises.
- Create a hierarchy of the identified triggers and rate them from least to most fearful.
- Start with the least feared exercise and have the athlete perform the task in a controlled and safe environment. Challenge the athlete to increase speed, repetitions and/or difficulty until they are performing without worry.
- Use goal-setting techniques, such as setting SMART goals (specific, measurable, attainable, relevant and timely), to create daily, weekly and monthly goals for building tools to manage anxiety and stress, as well as to do the identified fear exercises.
- Build coping skills to handle fear and worry triggered by pain and movement. Diaphragmatic breathing, positive self-talk and imagery techniques have all been shown to help reduce levels of distress, increase comfort and build confidence during rehabilitation and return to sport.
- Provide education about how fear and decreased confidence can increase their pain and get in the way of their ability to return to their sport.
Learn more and download tips for helping young athletes manage stress.
Psychology Services at Scottish Rite for Children
Our Psychology department has teams of pediatric psychologists at both our Dallas and Frisco campuses. Pediatric psychologists are embedded in the care of each patient, providing support to our sports medicine patients throughout their care and treatment. Learn more about our psychology services.
Emily Stapleton, Psy.D., is a pediatric psychologist at the Frisco campus of Scottish Rite for Children. She specializes in pain management, rehabilitation, coping with acute and chronic illness/injury and sports medicine. She has a particular interest in supporting young athletes following a sport-related injury.






.jpg?width=449&height=658 "A poster explaining the signs and symptoms of heat illness | Keep SIGNS AND SYMPTOMS OF HEAT ILLNESS Weakness Vomiting Excessive thirst Headache Fatigue Sweating Nausea Light-headedness cool when exercising in the heat Take rest and water breaks, every 15-20 minutes Avoid the hottest hours from 10:00 a.m. - 5:00 p.m. Drink a sports drink with electrolytes and 6-8% carbohydrates when training lasts over 60 minutes Avoid training in direct sunlight Take breaks in the shade Encourage removal of equipment during breaks (e.g. helmet) Wear loose-fitting, light-colored and moisture-wicking clothing SCOTTISH RITE FOR CHILDREN SPORTS MEDICINE (R Recognizing and responding to the signs and symptoms of heat illness is critically important. Though body temperature may be elevated, these may be present even when body temperature is normal. BE PREPARED Prepare ice and water before training sessions Limit caffeinated and sugary beverages Gradually increase physical activity in the heat Continue conditioning in the off-season Don't train in the heat while you are sick or have a fever Ways to respond quickly to signs and symptoms of heat illness: Full body immersion in an ice bath Iced-down towels applied all over the body 469-515-7100 scottishriteforchildren.org/sports")